“The most important lesson I learned in 2021 is that human beings can reconstruct their narrative with more ease than one might think; we just need to take the time to implement a few simple practices. Often, people in recovery harp on acceptance as the key to emotional health. But it’s important not to slide into resignation, expecting life to happen to us (as if we have no power over the outcomes in our life). Pain prompted me to seek out others who achieved the growth I craved – spiritually, physically, and financially. I observed what these spiritual titans were achieving and emulated their daily practices. With a bit of repetition, the changes were remarkable.”
Paul Manley, Executive Vice President & Partner at Driftwood Recovery, tells us why 2021 turned out to be his best year yet, and how we can all implement life-changing strategies to shift our narratives in 2022.
Spend enough time around someone who has a clear sense of who they are, and that infectious energy starts to rub off on you. The stories they tell about themselves and their comfortability with owning their identity have a sort of gravitational pull. The inevitable question becomes unavoidable: “If this person is so confident about who they are, what kind of person am I?”
Paul Manley is just this sort of person. His enthusiasm for self-improvement is magnetic. So, we were surprised to learn that he struggled to discover his sense of purpose in early adulthood. What prompted his shift from pain to progress over the past year? We asked him to share a few practices he established in 2021 that helped him level up to his next stage of spiritual healing:
Five practices that changed my life this past year:
1. Make time to understand what you want. When people set goals, their first mistake is not setting aside time to figure out what they want. It’s essential to be intentional. I’ve found journaling to be a valuable exercise for discovering short and long-term goals. I still set aside time in the morning to write down what aspects of my life I want to improve. Writing down my vision makes it more tangible and gives me a good jumping-off point. If I do not understand the desired outcome, I cannot create the road map to achieve my goal.
2. Make your vision clear. Once I determine what I want, I write my vision down in the form of an extremely specific intention statement. The vision statement helps me create a story of who I am that I can turn back to; this is the essence of my new narrative. Rather than writing “I want to be a person who….” I write, “I am a person who….” Wanting comes from a place of incompleteness but acting as if makes it so. Establishing this core sense of identity is essential because it reinforces the type of person you want to become.
3. Access your emotions. Ask yourself: How would I feel if I started to check off the goals on my list? Get as specific as possible. It helps me visualize myself taking small steps to accomplish my vision: what my environment looks like, what thoughts I might have about myself, what I’m wearing, etc. When I have difficulty accessing the emotions related to a specific goal, I turn to intentional meditation to access my gratitude for every stage of the journey. Taking that extra time to get quiet and turn inward allows me to feel whole and appreciate every step along the way.
4. Put your intention statement somewhere you can see it. Create a visual cue to accompany your vision you can review every day, multiple times a day. This visual stimulus is critical because what catches your attention creates intention. Placing my intention statement in plain sight allows me to stay grounded in the outcome and not lose sight of the result. Understand that your goals may change along the way; what’s important is the feeling that the intention statement elicits. I hang up words and pictures on my bulletin board that define success for me: adventure, love, leadership, and so on. These are values that I can aspire to every day that make me feel more complete.
5. Remember: structure comes before freedom. Long-term growth does not always produce immediate results. I must establish the routine of acting before starting to feel the benefits. The most effective change comes from repetition. It’s a common misconception that structure and routine are the antitheses of freedom. In reality, structure begets freedom. When every action comes from genuine intention, you create meaning in the mundane and free yourself from practices that no longer serve you. I have also found that when I am consistent with structured spiritual practices, my relationship with time changes. It no longer feels like there are not enough hours in the day. Instead, things start to fall in place with exceptional timing.
Driftwood’s Culinary Director, Jason Donoho, provides us with festive mocktail recipes as we plan for the holiday season.

Pear Rosemary Tonic
Ingredients
● Ice as needed
● 2 oz Pear Rosemary Syrup (Combine 1 diced pear and 2 sprigs of fresh rosemary with 2 cups water and 2 cups sugar. Bring to a simmer and let infuse off the heat for 30 minutes. Strain and store in the fridge for up to 30 days.)
● 1 oz Fresh Squeezed Lemon Juice
● Fever Tree Tonic Water or your favorite brand to Top
Instructions
Combine all ingredients in the order listed in a glass filled with ice. Garnish with a lemon wedge and a sprig of fresh rosemary.

Ginger Orange Punch
Ingredients
● Ice as Needed
● 2oz Fresh Squeezed Orange Juice
● 1oz Ginger Simple Syrup (Combine 1 cup peeled fresh ginger slices with 2 cups water & 2 cups sugar. Bring to a simmer and let infuse off the heat for 30 minutes. Strain and store in the fridge for up to 30 days.)
● Ginger Beer or Ginger Ale to Top
Instructions
Combine all ingredients in the order listed in a tall glass filled with ice. Garnish with an orange twist.

Spiced Coconut Golden Milk
Ingredients
● 1 Can Full Fat Coconut Milk
● 1 tsp Turmeric
● 1 tsp Cinnamon, Ground
● 4 Tbsp Honey
● 1 pinch Sea Salt
● 1 pinch Freshly Ground Black Pepper
Instructions
Combine all ingredients with a whisk in a small saucepan and bring to a simmer, careful not to boil. Serve warm in a mug with a sprinkle of ground cinnamon to top.

Pineapple Coconut Mojito
Ingredients
● Lime juice as needed for the rim of the glass
● Coconut Flakes as needed for the rim of the glass
● 4 sprigs of fresh mint leaves
● 2 oz fresh lime juice
● 4 oz fresh pineapple juice
● 4 oz Coconut Water
● Ice as needed
Instructions
Dip the rim of a glass in lime juice and then the toasted coconut, fill with ice. Place 4-6 fresh mint leaves at the bottom of the glass with the lime juice and muddle to lightly crush the mint. Add the coconut water and pineapple juice. Garnish with a lime wedge and a sprig of the mint.
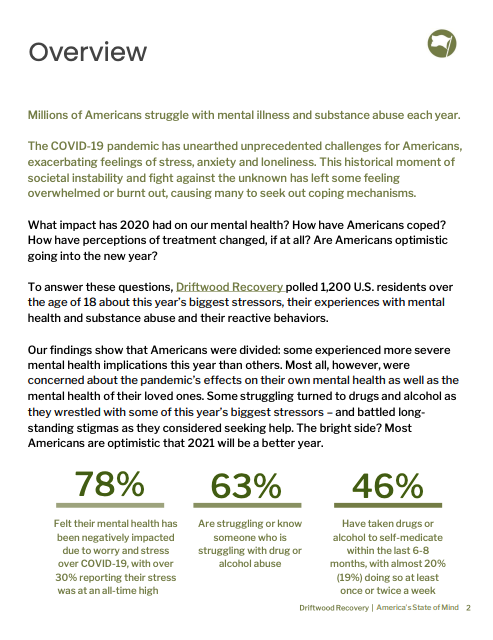
A Pulse of 2020’s Impact on Mental Health in the U.S
“As human beings, we experience difficult emotions—sadness, anger, disillusionment—when faced with a traumatic experience. Giving ourselves permission to feel these emotions and seeking support to help us cope with them are important tools to develop resilience.”
Resilience is one of many psychological concepts that has been given a great deal of attention in recent years. All you have to do is Google “resilience,” and the first article that appears organically is “Building Your Resilience,” written by the American Psychological Association (APA), followed by many other how-to articles. Since mental health has become commonplace conversation and something that even some public figures are opening up about, self-empowerment through resilience has become ubiquitous. The strength of the human spirit in the face of adversity is an enigma that we as human beings long to understand. Our very own Dr. Vanessa Kennedy, PhD, told us what resilience means to her, some examples from her personal experience, and five myths she commonly sees associated with the subject. Her thoughts were also featured in a FAST COMPANY article.
PM: How would you define resilience?
VK: Resilience is the process of coping well with adversity and moving forward in an adaptive way. When we face challenges, loss, or traumatic experiences in our lives, we may subscribe to some common myths about resilience when struggling to make sense of our overwhelming mix of emotions.
Q: How could one practice resilience within their own life?
VK: Resilience involves coping with the aftermath of an event, but it is also about preventive care and wellness. Cultivating positive thoughts and supportive relationships goes a long way in helping us to deal with challenges when they arise. When we can focus on solutions, immerse ourselves in activities we enjoy, build trust in our relationships, and have a sense of meaning and purpose in our lives, we have laid the groundwork for handling a difficult experience.
PM: Do you have a quote to sum up resilience?
VK: A mindset that empowers us to look at adversity as an opportunity to grow and change is beautifully demonstrated by the Latin phrase “succisa virescit,” which when translated states “that which gets cut down, grows back stronger.”
PM: Can you give any examples of resilience from your personal or professional life?
VK: I worked at the Menninger Clinic for 8 years in Houston, TX, where I was born, raised, and attended college. My parents live in a suburb of Houston, as did two of my siblings and much of my extended family. My whole life was essentially rooted there. Selling our house in Houston and moving to Austin, TX, with my eight-month-old baby boy, an eight-year-old stepdaughter, and a new job with a residential treatment center that wasn’t even officially open yet definitely required resilience! I needed to feel the stress mixed with excitement mixed with sheer terror of helping to get a new program off the ground and create something meaningful. I relied on established support from friends and family back home cheering me on, as well as the hope, creativity, and enthusiasm of the new team of caring individuals I met, who wanted to build a unique place that would benefit others. I feel very grateful to have adapted to a major transition in my life. I’ve been able to cultivate work relationships with new people who helped me to grow and change, and the experience has allowed me to evolve into a more versatile and independent version of myself.
PM:What are the common myths about resilience you see?
VK:
1) “I need to be strong.”
The process of resilience involves distress. As human beings, we experience difficult emotions – sadness, anger, disillusionment – when faced with a traumatic experience. Giving ourselves permission to feel these emotions and seeking support to help us cope with them are important tools to develop resilience.
2) “You either have it or you don’t.”
Resilience is not a genetic trait. While research suggests that confidence in your abilities and problem-solving skill are key ingredients in developing resilience, these elements can be learned and cultivated through the encouragement we receive from others, the actions we take, and the way we choose to think about our distress.
3) “I should be able to do this on my own.”
Research shows that resilience is just as much about having supportive relationships as it is about our internal strengths. Opening up about how we are doing, allowing others to help us, or watching how others have coped with adversity can remind us that we are not alone.
4) “I should feel better by now.”
Having resilience is not like turning on a light switch. It may be more like strengthening muscle groups in the body – there may be some areas of life that improve while others may take more time or effort. For example, a person who loses their home to a fire may furnish a new home, but it may take much longer to emotionally accept the loss or help family members adapt.
5) “I want things to be like they used to.”
Some adverse or stressful events may change things so that they do not go back to “normal.” Adapting involves developing a “new normal” in which we can evolve and even thrive. Divorce, moving to a new place, obtaining a life-altering injury, or losing a loved one are examples of events that change our world permanently, but can present an opportunity for growth.
Links Related to Article
Fast Company: These 5 Myths About Aging Might be Hurting Your Ability to Cope
An Interview With Peter Fonagy on Building Resilience
“We truly have seen the contagiousness of personal development, and when more people engage in personal development, more people begin enjoying life”
It is said that crises can create opportunities. External pressures can bring companies to a turning point, after which, they either mature into organizational health or begin to disintegrate.
At Driftwood Recovery, a series of constructive crises (including a period of unexpectedly fast growth, a leadership restructuring, and a global pandemic) got CEO Peter Fluor, COO Brad Kennedy, and Executive Vice President Paul Manley thinking about the treatment center’s organizational wellness. The three began meeting every week, Manley says, to discuss and re-evaluate organizational goals, to exchange ideas candidly and constructively, and make sure that Driftwood’s culture is healthy.
Perhaps one of the most beneficial things for the organization has been the leadership team’s journey to personal development through individual therapy and team/group therapy. “We truly have seen the contagiousness of personal development, and when more people engage in personal development, more people begin enjoying life,” touts Manley. “Peter got us to start working with a pHD named Ted Klontz, who holds a monthly phone session and a quarterly in-person intensive to insure clear lines of communication.” Having a clinician objectively orchestrate their relationships on both the personal and professional level has allowed them to become a much more congruent team.
In the past, Fluor says, he sometimes found himself “witnessing, and therefore participating in, a fear-based culture: one where people carry out tasks because they’re afraid of what will happen if they don’t, and not because they’re taking ownership of their work.” At Driftwood they work hard to give everyone a voice, and avoid micromanaging. “We want people to use their creative freedom to contribute to the program’s success, to weigh in on whatever the objective is. The leadership team gives people a direction, and then they run with things, put their own spin on them, get excited about what’s in front of them.”
Early in Driftwood’s life, Manley says, “I was spending so much time at work, or thinking about work, that I couldn’t talk about anything but work; it was my entire identity.” That kind of focus is unsustainable over the long run; managers that demand it of themselves will burn out; managers that demand it of their employees are signing up for long-term organizational instability. He and the other members of the leadership team are taking steps, he says, to ensure that everyone at Driftwood can develop both within and outside the company. (Alumni Coordinator Nick Borges, for instance, is working toward a master’s degree in social work while he works at Driftwood.)

“One moment that stands out is a Driftwood family-weekend workshop,” Kennedy says, “we were all introducing ourselves to the visitors, and Danielle Cobb, our Lead Care Coordinator, started describing Driftwood’s take on attachment based treatment. I thought: how cool is that? I’d never worked in a place where the direct care staff was given the chance to articulate the clinical philosophy so well, and I saw that our staff members were finding their voice.”
Moments like those are the result, Kennedy says, of eliminating unnecessary hierarchy in the workplace. “Certainly, we all have different roles to play,” he says. “But we’re a team. Everybody’s voice matters. And just as we want to know, understand, and accept all of our clients, we want the same for our staff. We want to deeply understand the people we work with—to collaborate enough that we can, for instance, design a growth plan with them in mind that benefits both them and the organization.”
During weekly leadership meetings, Manley says, “a majority of our conversations are about the staff: how we can help them, how we can empower them. Brad is always looking at training opportunities for the clinical & care coordinator staff, and he has done a great job at creating space for the staff to have a weekly process group, so that we can match the intensity of the work we are asking our clients to partake in.”
“I think we’re doing a pretty good job,” Fluor says, “of remaining principled and remembering our collective purpose. When we get off-track, we hold one another accountable. When we disagree, we look for advice from a neutral third party.”
“If we get preoccupied with some sort of internal competition,” he says, “we’re totally missing the point. We’re here to be a resource for people who are struggling. If we are distracted by some sort of turmoil, we’re not being of maximum service.”
The three have brought past experiences from previous organizations and have tried to mold a culture based on a majority of the pros, while leaving behind the cons. Fluor says he’s been “amazed by the productivity and the sense of accomplishment, the comfort and the camaraderie that’s created when people feel trusted and respected.” The three are now looking to create a program manual in order to share their journey, organistructure and give an inside view to the culture they feel so fortunate to be a part of.
Links Related to Article
Organizational Health: A Fast track to Performance Improvement
Harvard Business Review: The Culture Factor
Forbes: Why Culture is Becoming More Important
Inc: The Importance of Building Culture In Your Organization
“When you find your tribe, you can rely on people—and you have to show up for them”
This is the eighth in a series of posts introducing the people who make up Driftwood Recovery’s community of caregivers.
Through these conversations, you’ll get a chance to meet the people on Driftwood’s team—from its executives to its care coordinators. You’ll learn about the programs they facilitate, and about how their work serves Driftwood’s overall treatment philosophy. You’ll learn about the various paths that brought them here. And you might pick up a book or Austin restaurant recommendation.
In this post, Kuraĝo editor Matt Williamson talks with Driftwood’s Alumni Coordinator, Nick Borges.
***
Matt Williamson: You had kind of an interesting path to your current job here at Driftwood.
Nick Borges: I used to work in corporate finance. I came to Austin to go through treatment. I knew, when I got out, that I didn’t want to be in finance at all. I’d always been a foodie, so for the short term, I figured I’d do some sort of restaurant work.
I was initially hired here at Driftwood as a sous chef. I worked in the kitchen for about eight months. During that time, I had a lot of one-on-one contact with the clients: getting to know them, giving them feedback about my own recovery—what’s worked for me, what hasn’t worked.
In that eight months, I figured out that direct care was the path for me. I got a job offer from another company in Austin; I’d be managing all of their sober living facilities. And I was going to accept it.
The Monday after I put my two weeks in, Peter Fluor sat me down and said, “Listen, what do you want to do?” I hadn’t had that initial conversation with him. I told him that I wanted to go into direct care, that I wanted to be more involved with the day-to-day operations, to be in the trenches a bit more. And he said “What if you became Driftwood’s Alumni Coordinator?”
I didn’t even think about it. I said: “absolutely.”
MW: Did you know what the job title entailed? Is “alumni coordinator” a position at other residential recovery places?
NB: At the good ones, yeah. I knew a little bit about the job just from my own experience in treatment. But I knew that a lot of things needed to happen at Driftwood that weren’t happening elsewhere.
I was going to be the first Alumni Coordinator here at Driftwood, so the scope of the job was open to some extent, and I was able to build the program.
MW: Without throwing anyone under the bus . . . what are some of the things you thought Driftwood should do that other places weren’t doing?
NB: I think the biggest piece is the continual support that’s provided after you leave treatment.
My own experience after completing treatment was that I got one call from the alumni coordinator. I never heard from him again. There was also a calendar of events that was emailed to me. That was the extent of my contact with the treatment center.
MW: It sounds like the kind of contact you’d have with a college you graduated from. You get the alumni magazine, and an occasional call reminding you about the five-year reunion.
NB: Yeah. We wanted to do something totally different. Once a person comes to Driftwood—whether they’re a resident, a former resident, a family member of a resident, or a staffer—we want them to feel like they’re permanently part of our community.
My part of that is to provide three kinds of opportunities for alumni: opportunities to be of service to others, opportunities to have fun in recovery, and opportunities to find fellowship.
MW: Can we talk about all three of those separately? What’s the service component?
NB: We’ve set up alumni groups, chapter groups, in Houston and Austin, and we’re working on starting one on the west coast. The Austin group comes out to Driftwood regularly—they bring a meeting to the residents, and come out and have dinner with them. Alumni get to know the residents and provide a sense of what recovery looks like outside of the gates of treatment.
That’s one aspect of service. And next weekend, for instance, we have Recovery in the Park. It’s an event that takes place every year during Recovery Month. A bunch of people who have gone through recovery or who work in recovery get together for food, music and fellowship. But we try and stay involved with all kinds of service projects in and around Austin.
MW: The second element of your job—helping alumni have fun—might sound less important to some people. But my impression, from talking to younger alumni here in Austin, is that it’s a big deal.
This city really emphasizes drinking. Austin brands itself as “the Live Music Capital of the World”—and getting drunk or high is part of the typical experience of going to shows—so drinking, implicitly, is part of Austin’s official identity. It seems natural for young people in cities like Austin or Portland or Miami to worry that being sober means that they’ll be excluded from most of the exciting things that are happening in town, that they’ll be excluded from the places where young people congregate.
NB: “How the hell am I going to have fun?”
The cool thing, to me, is that once you remove the drugs and alcohol, people find things that they never thought were fun before. They’re open to new experiences. They start rediscovering old interests.
The Driftwood alumni group goes to concerts, to dinners. We go rock climbing, and to the climbing gym. Hiking, kayaking. I try to go to Houston every month to meet the alumni chapter there. Last month, we all went out to the Astros game.
Austin does have this kind of connotation of a party scene, and drugs and alcohol are involved in fun in the city. But on the other side, Austin’s got the reputation of one of the best places to be in recovery. You can always find people who are trying to have fun without drugs and alcohol.
MW: I was talking to an alum about “the fear of missing out,” and how it motivates people to keep drinking and using. But then, if you’re drunk and high all the time, you’re missing out on everything other than being drunk or high.
NB: Whenever people ask “how am I going to have fun without drugs and alcohol?”—well, most of the time, you weren’t having fun when you were using anyway. “Fun” is going to look a lot different than it did before.
MW: The friendships people form when they’re sober are probably very different from the friendships people form when they’re drinking.
NB: When you’re relying on alcohol to get you through your social life, you might be hanging out with people you don’t even like—or who don’t know the real you. When I was using and drinking, I was so far from my true self that I was basically projecting a different person. And that projection was attracting people very different from the ones I really wanted to be around.
From the beginning of my recovery, I’ve made relationships that are so strong, and genuine, that it’s hard to compare them with any relationships I had before getting sober. I still have strong friendships with folks I grew up with, but even those relationships look a lot different than they did before I got into recovery.
MW: I guess that brings us to the third opportunity you mentioned: the opportunity for fellowship. Could you explain the categorical difference between “fellowship” on the one hand,’ and “fun” and “service” on the other?
NB: You find fellowship through service and socializing, so they’re related. But “fellowship” can mean going to a support meeting. It means being around like-minded people who understand your struggles and share some of your goals. We have a term in the recovery community “family of choice.” It’s like finding your own tribe.
When you find your tribe, you can rely on people—and you have to show up for them. You have a group of people who are going to call you on your bullshit when you need to be called out. People who are going to hold you accountable.
MW: You’ve talked a lot about the ways that you’ve grown since becoming sober. Can you share something that you’ve learned specifically from your work at Driftwood?
NB: So in addition to serving as Driftwood’s Alumni Coordinator, I work in Admissions, and I’m part of the Family Program team. When people come in, I’m often the person who walks them through the whole intake process. So a lot of my job involves working with the families of residents: talking to them, listening to them, and applauding them for taking this step for a loved one. Those conversations, and the ones I have with people participating in Driftwood’s family programming, really bring home why I’m here: to make sure that the alumni can thrive after they get through their initial treatment phase here.
This disease affects the entire family, not just the person who’s suffering directly from addiction.
If people are abandoned after treatment—or if they feel they’re drifting further and further from the community that helped them get sober—they’re at a much higher risk of relapse. As Alumni Coordinator, I’m helping people consolidate the gains they’ve made: turning this from a 30-day recovery process into a permanent recovery lifestyle.
I should mention also that this work has been enormously helpful in my own recovery.
MW: How so?
NB: Being a resource for people whose sobriety is fragile forces me to put that much more emphasis on my own recovery, so that I can show up in a good way for the people who depend on me. In general, meaningful responsibility helps you stay sober.
MW: I’m not sure I know anyone who’s juggling as many responsibilities as you are right now. Apart from your work life, you’re insanely busy.
NB: Yeah—I just finished my first semester in Texas State’s Masters of Social Work program. It’s a full-time program. Driftwood’s supporting me through the process—structuring my work schedule around my weekday classes.
MW: Is your plan to stay at Driftwood after you graduate?
NB: Absolutely. I love direct care. And I want to stay with the community integration piece of Driftwood’s program: working with people as they transition from residential care into healthy independence—helping people become their best selves, and thrive in life, through all stages of recovery.
Nick Borges, Alumni, Long-Term Recovery, Family
“The critical thing is to face our fears—to stay with an emotion we’re having difficulty with, or to stay with the physical pain—and discover: everything’s impermanent; this doesn’t last forever.”
Breaking the Pain-Fear-Avoidance Cycle
Pain has an element of blank;
It cannot recollect
When it began, or if there were
A day when it was not.
—Emily Dickinson
The onset of chronic pain can be, in the words of one Driftwood alumnus, “soul-crushing.”
Pain makes the sufferer’s world smaller. It intrudes on relationships, from the most casual to the most intimate. And when a doctor tells a patient that the pain is unlikely to subside—or can be managed only with drugs that cloud the mind—one natural reaction is despair.
All of these are reasons why people living with chronic pain are at a particular risk of retreating into addiction.
***
“Many pain treatment programs,” according to Dr. Ron Siegel, “take the attitude: ‘let’s first try to resolve your pain—including, historically, with the use of opiates. Once you feel better, we can work on rehabilitation, can make you physically stronger, can help you engage more fully in your life.’ Meanwhile, the research is pretty overwhelming: approaching chronic pain from this angle doesn’t work very well.”
Dr. Siegel—currently Assistant Professor of Psychology at Harvard Medical School, and a board and faculty member at the Institute for Meditation and Psychotherapy—advocates for a different strategy, one that “draws upon cognitive, psychodynamic, and behavioral techniques along with mindfulness-based exercises, combined with everything we know about aggressive rehabilitation.”
“Almost everybody who’s caught in chronic pain syndromes,” he says, “has fallen into some degree of what we call kinesiophobia: the fear of movement. Whether it’s because of medical advice, or because they’ve noticed that certain activities seem to hurt, they start avoiding activity in the hopes of feeling better.”
Sedentariness causes deterioration. As Driftwood Wellness Director Connie Cole put it last month: “If you’re not moving every day, you’re degenerating.”
Inactivity “makes people anxious about using their bodies normally,” Dr. Siegel says. “Pain sensations,” in turn, “are amplified by fear,” creating a kind of feedback loop.
“If you put somebody’s hand in ice water, and you tell them that they’ll have to keep it there for thirty seconds, and you ask them, after fifteen seconds, to rate their pain, they’ll say: ‘It’s not too bad.'” When a person is instead told that their hand must stay in the water for ten minutes, “they’ll tell you after fifteen seconds: ‘it’s freezing! This already hurts.”
To find lasting relief from isolating, debilitating pain, people must refuse to be governed by fear.
***
Dr. Siegel is the author of several acclaimed books—some for lay readers, others for professionals—on mindfulness, psychotherapy, and mind-body treatment. Since late 2019, he has consulted periodically with Driftwood Recovery’s clinicians, helping them create individualized programs of recovery for people with co-occurring pain and substance abuse disorders.
“On a case-by-case basis,” he says, “we consider the factors and forces that are creating the chronic pain for an individual. We pay close attention to the individual’s personal history, family background, psychological dynamics, cultural background and physical condition: any challenges that might relate to the chronic pain, or to possible pathways out.”
Those pathways typically begin with a concept familiar to anyone who has spent time at Driftwood: courageous surrender.
“Pain times resistance equals suffering,” Dr. Siegel says. “This turns out to be the case across the board: not just with pain disorders, but with virtually all psychological difficulties.”
“Say a person is struggling with anxiety. If the person is willing to feel it—to accept anxiety but participate fully in life—their life is not derailed. But if they, for example, refuse to fly on airplanes because they don’t want to feel anxious—well, then, they have an anxiety disorder. Our attempts to avoid discomfort are at the heart of so many of our problems.”
Nowhere is this truer than in the realm of addiction. “Virtually all substance abuse disorders,” Dr. Siegel says, “involve turning to a substance to avoid feeling something unpleasant.”
***
Your pain is the breaking of the shell
That encloses your understanding.
—Khalil Gibran
“The reason mindfulness practices are proving to be so helpful for such a wide variety of psychological difficulties,” Dr. Siegel says, “is that they turn our attention toward whatever we’re experiencing, whether that be physical pain, or sadness, or fear, or joy, or love or appreciation.”
“It’s about opening to experience.”
“The vast majority of chronic pain,” Dr. Siegel says, “has a big psychological component.” In the case of back pain—the subject of Siegel’s bestselling Back Sense—there is surprisingly little correlation between reported pain and the physical problems revealed by MRIs. Many people have bulging or herniated discs, but claim that they have never experienced more than two consecutive days of back pain. “In other words: people who are pain-free often have the spinal abnormalities we point to as the cause of pain.” On the flipside are the “countless patients” who have gone through successful back surgery, but find that their pain persists.
“The therapist’s task,” in such cases, “is to figure out what other process is causing chronic muscle tension, preoccupation with a particular part of the body, and the withdrawal from normal activities that can cause stress and depression, that can tank a life.”
Mindfulness-based therapies, Dr. Siegel says, can break the “pain-fear-avoidance cycle.” With pain management—as with addiction treatment—meaningful recovery begins with acceptance and psychoeducation: “Understand what’s keeping you trapped in your difficulty. Understand how your mind and heart work. Chances are, you’ll end up saying: ‘Oh, I see. The coping strategy that I’ve been using doesn’t work very well.'”
The search for a replacement strategy is, in a sense, a search for new resources.
“That search can start at a place like Driftwood, with the support of a new community that reassures us what we’re going through is okay. It can start with self-soothing strategies like talking to a friend, or getting a massage, or being in nature.”
“The critical thing,” Dr. Siegel says, “is to face our fears: to stay with an emotion we’re having difficulty with, or to stay with the physical pain, and discover: ‘everything’s impermanent; this doesn’t last forever.'”
“It’s your knowledge that you can take on a frightening challenge—that you can enter a wave of pain, pass through, and come out on the other side—that will give you the strength to free yourself.”
***
Watch:
· The Science of Mindfulness, Dr. Ron Siegel’s introductory lecture on mindfulness-based psychotherapy, which has been viewed more than 360,000 times
Listen:
· A collection of recorded meditations recommended by Dr. Siegel
· Jake Knapp’s interview with Dr. Siegel on the popular podcast The Science of Success
Read:
· New research indicates that even a 30-minute introduction to mindfulness can significantly relieve pain: “It’s as if the brain were responding to warm temperature, not very high heat.”
· As doctors become more interested in mindfulness-based solutions to health problems like hypertension, “scientists [may] need to develop new metrics to analyze a potential medical intervention . . . rooted in ancient Buddhist philosophy.“
· A JAMA study finds that “an online version of mindfulness-based cognitive therapy” may aid in the treatment of anxiety depression.
· Mindfulness training for children is gaining traction at home and at school.
“In some ways, a person who comes through a program like ours has an unfair advantage over the general population. Because people don’t ordinarily get that education in coping with life. We’re not born with a manual.
“Every Time I Teach, I Learn”
This is the sixth in a series of posts introducing the people who make up Driftwood Recovery’s community of caregivers.
Through these conversations, you’ll get a chance to meet the people on Driftwood’s team—from its executives to its care coordinators. You’ll learn about the programs they facilitate, and about how their work serves Driftwood’s overall treatment philosophy. You’ll learn about the various paths that brought them here. And you might pick up a book or Austin restaurant recommendation.
In this post, Kuraĝo editor Matt Williamson talks with Driftwood’s Medical Director, Rey Ximenes, MD.
***
Matt Williamson: You have several board certifications, correct?
Ray Ximenes: Well, I have a board certification in anesthesiology, which is where I started. And then I got board certifications in pain medicine and interventional pain medicine. And then I got board-certified in acupuncture and in naturopathy. My last board certification is in addiction medicine.
MW: Could you explain the difference between pain medicine and interventional pain medicine?
RX: Pain medicine is what we all started out doing. It was basically using what we had—mostly opioids—to treat pain. We’ve since gotten into different drugs and medications: gabapentin and muscle relaxers and antidepressants and things like that.
In interventional pain medicine, we use nerve blocks. That means, for example, using a local anesthetic to dull a nerve’s ability to transmit information. We also use steroids to calm inflammation. And we use spinal cord stimulators and intrathecal pumps, pain pumps. We’ll perform what I guess is called “minor surgery,” although that term—“minor surgery”—I’m never sure quite what it means.
MW: Kind of an oxymoron.
RX: Exactly.
MW: So in interventional pain—correct me if I’m wrong—it sounds like one distinction is that you’re not using drugs as often?
RX: Not as often, no.
MW: And the approach sounds much more localized, or targeted. I can see the connection to acupuncture.
RX: Acupuncture is, for me, just another tool. For years, I saw people doing epidurals and facet blocks and radiofrequency thermocoagulation. And I thought: no one’s doing acupuncture. I realized that if I did that, I’d be ahead of the crowd.
MW: Why do you think that this treatment, which is so mainstream in half of the world, has been so slowly adopted in the West?
RX: It’s hard to really know. Back in the day, the Emperor of China wanted to trade with the West. And at a certain point, he actually said: “No more acupuncture. No more Tai Chi. No more Chi Gong. It’s all this magical stuff that makes people think we’re country bumpkins.” They started adopting a lot of Western medicine at that time, and really put down and shunned traditional Chinese medicine. When Mao took over, I think he kind of went, “This Western stuff’s pretty expensive. We’ve got to figure something else out.” He wanted to go back to some the old ways, including acupuncture and herbs.
In the Western world, we think acupuncture is this thing unto itself. We address it as acupuncture, and we have licensed acupuncturists. In the East, they’re kind of scratching their head about that, because traditional Chinese medicine has always included ten or eleven different disciplines. Diet is very important. Exercise is very important. Herbs are of paramount importance. Acupuncture is important, but it’s part of the fine tuning, not the primary thing. Somehow we got fascinated with the art of needles. An acupuncturist here is kind of like a mechanic who’s licensed to use one specific type of socket wrench.
I use acupuncture as a tool. I also use herbs as a tool. I use a lot of exercise. I use Tai Chi and Qi Gong. And I use a lot of lifestyle advice: telling people what to eat, how to eat. It’s truly a holistic approach.
MW: Do you ever teach Tai Chi to residents here at Driftwood?
RX: Yeah.
MW: I assume that most people who stay here don’t have any experience with it. How do they usually take to it?
RX: Honestly, it’s tricky. Nobody’s here long enough to really learn it very well. So what I finally did was to set up weekly lessons at Bull Creek Park. I said: “Look, everybody’s invited, every Saturday morning.” It’s very much the Eastern way of teaching Tai Chi: “just show up at the park and do it with us.” And eventually you will learn.
MW: It strikes me that Driftwood is a small, intimate place. The resident-to-staff ratio is 1-to-2.8; by design, there are almost three people on staff for a single resident. And at the same time, people are coming in with a wide variety of substance abuse and pain problems, and their recovery programs are highly customized. I would imagine that, for the medical staff here, this would present a challenge. You see a little bit of everything, right?
RX: Sure. People come in here and need something very specialized. For example, if someone is withdrawing from alcohol, we’ve got to be careful. We’ve got to really monitor them, and make sure that we have every medication on hand that we could ever need, because one of the problems people have with alcohol detox is they can get into seizures. At the other extreme, when someone has been dependent on hallucinogens, most of the withdrawal is psychological; there’s no full-blown physiologic detox, although symptoms can recur for a long time. You have to look at each person and know what you’re doing with each one.
Anyway: once you’re in the clear, out of your early withdrawal, the approach to treating addiction is similar for everybody. Obviously, there are nuances that are different for each individual. But in the end, the goal of an addiction specialist is to make sure the person is healthy.
MW: When you’re speaking to somebody who has never had a problem with substance dependency—is there some sort of analogy you typically use to help them understand what an addicted person is experiencing? Why is it so hard to “just quit?”
RX: I do have a favorite analogy, actually.
First off, know that addiction takes over the survival center of the brain. I don’t call it the “pleasure center”; it’s the survival center.
There’s a cup of coffee on the table here. Let’s imagine that I told you to take a sip of that coffee, and you didn’t want to. If you felt strongly about it, you’d refuse.
Now: what if I took a .45 out and pointed it at your head and said: “take a sip of the coffee?” What are you going to do?
MW: Take a drink.
RX: That’s what the addict is experiencing in the brain. “If I don’t drink that, if I don’t snort that, if I don’t shoot that, I’m going to die.” The addict might know that they don’t have to. But they feel that they do. And that’s the trap.
MW: Listening to you, I was just reminded of a documentary I saw recently about a treatment center in Alberta. It’s a public, free, seemingly high-quality residential treatment program. In one scene, this guy comes in who seems, genuinely and desperately, to want help. A staffer is explaining to him what he has to do to get into the program. “It’s free, we’ve got a place for you, we’ll just sign you up. The only thing is, you have to abstain from drugs for five days before you enter treatment here.” And the guy seeking treatment says, basically, “forget it. I’ll never be able to do that.”
RX: That’s pretty rough.
MW: You can see that he isn’t even contemplating it. He’s just listening politely after he hears that “five days” is a hard requirement. In the next scene, a different guy is explaining that he would rather die than go through the agony of fentanyl withdrawal.
RX: That five-day period is going to feel like five days of re-enacting The Deer Hunter. Click. Click. Click. Five days of that? You can’t do it. That’s where residential treatment becomes crucial.
Once you get through early withdrawal, though, you’ve come to the most important part of recovery. When you reach that point, what often matters more than anything else is community. You need a group of like-minded people around you, who know something about what you’ve gone through and are going through. Every time you want to go back and use, there are people who are right there, ready to say: “Nah, man. Don’t do that. I did that. Here’s what happens.”
At Driftwood, we keep people busy, and we educate people. I tell people that this is an educational program. Using cognitive behavioral therapy or motivational interviewing, or various other techniques, we’re teaching you how to cope with life events. Because in the end, addiction is about what you’re hiding from. What is it you fear? If we can get people to cope with that fear in a healthy way, then we’ve made it.
In some ways, a person who comes through a program like ours has an unfair advantage over the general population. Because people don’t ordinarily get that education in coping with life. We’re not born with a manual.
MW: You’re talking about skills that everyone needs. But we don’t develop them, because we’re not in crisis situations that force us to develop them.
RX: Why don’t we have seventh-grade AA? Some kind of cognitive behavioral class: Life 101? We pretend like it’s not necessary until it is, and by that time it’s almost too late.
MW: Most people either have incoherent value systems, or they simply haven’t thought about what their values are. We’re nose-deep in this culture that trains us to laugh at the idea of ever getting reflective, philosophical.
RX: Yes, and getting into recovery presents opportunities to inquire, to grow. I’ve learned so much doing addiction medicine. I’ve learned so much about myself. I’ve started paying more attention to the ways I deal with things.
The original meaning of “doctor,” you know, is “teacher.” And so I come out here every week, and I teach. And every time I teach, I learn.
“At Driftwood, the staff and residents always eat meals together, we do a lot of things together, and we don’t ever want the clients to feel like the staff is separate from them. It’s very integrated. We know so much about every client, and work so much on each case. We get creative with every treatment plan, with every discharge plan.”
“No One’s Ever Going to Be Just a Number Here”
This is the fifth in a series of posts introducing the people who make up Driftwood Recovery’s community of caregivers.
Through these conversations, you’ll get a chance to meet the people on Driftwood’s team—from its executives to its care coordinators. You’ll learn about the programs they facilitate, and about how their work serves Driftwood’s overall treatment philosophy. You’ll learn about the various paths that brought them here. And you might pick up a book or Austin restaurant recommendation.
In this post, Kuraĝo editor Matt Williamson talks with Driftwood’s Lead Care Coordinator, Danielle Cobb.
***
Matt Williamson: How many care coordinators do you supervise?
Danielle Cobb: Seventeen at the moment.
MW: Were you a care coordinator when you first started working at Driftwood, or were you hired as a supervisor?
DC: I was a care coordinator. About a year ago, the leadership team here took a chance on me.
MW: And since then, you’ve done all of the hiring, the training, the supervision?
DC: Yes—and also a lot of what I would call “coaching.” Encouraging people to develop professionally, doing what I can to help them achieve their own goals, to get to the place where they want to be in the future.
MW: It seems like the care coordinators do a bit of everything here. I think the impression anyone would get, even walking around the campus as a guest, is that the care coordinators are the people who make this place run.
DC: In some ways, the people I supervise have the most difficult job at Driftwood. They’re here when therapists aren’t—including in the evening, obviously. They offer support in any way that they can: making sure that residents get to meetings on time—and just doing anything and everything that turns out to be necessary on a given day.
MW: How much communication do care coordinators have with the therapists here?
DC: A lot. We do shift reports: the morning shift report, the afternoon, evening, and then the overnight shift report. I also attend Driftwood’s morning meeting, where all of the clinicians are present, so I get a chance every day to bridge the gap of communication between the therapists and care coordinators.
MW: If this question isn’t too open-ended or tedious: could you walk me through all of the different interactions that a resident might have with care coordinators over the course of a day—from the time when they wake up to the time when they go to sleep?
DC: We come on at seven and wake everybody up. We have a communal breakfast with the residents. Then there’s a bit of exercise time and some personal time for the residents. After that, we help people get to their therapeutic programming. There are group sessions running back-to-back through the morning. Through that part of the day, our job mostly involves shepherding people from one group to the next—pulling people in and out of groups for individual therapy, appointments, massages, things like that.
After lunch, there’s more programming, and a couple more groups. And then residents either do group exercise, or an experiential activity off-property. That could be kayaking, yoga, paddleboarding, hiking, bowling, rock climbing—you name it, we do it all.
We have a communal dinner. And then residents have a bit of down-time between dinner and the night’s AA meeting, which is off-property.
MW: What meetings do residents go to? Are they in Austin?
DC: A lot of the time, yes. The location varies. The care coordinators confer and make a decision based on the needs and interests of the residents who are staying here.
A lot of the staffers here are in recovery. We’re familiar with the meetings around town, and we know what meetings are likely to be most beneficial for the clientele that we have currently. Maybe we have a lot of older clients, so we’ll take them to a meeting with people they might relate to. Or maybe we have a lot of young clients and we want to get them involved in a younger community, in which case we’d likely take them to a meeting in the city.
MW: And then finally, you’re back at Driftwood—
DC: And it’s wind-down time. We have tea and group meditation right before bed.
MW: You mentioned that many of the care coordinators are in recovery. Some of the alumni I’ve talked to have mentioned the importance to them of being cared for by people who have gone through many of the same experiences they’re going through.
DC: Sure. But what makes Driftwood special isn’t necessarily that most of us have experience with some sort of recovery path, but the culture here. The love and support and connection and community we have here is unlike anything that I experienced in treatment. It’s unlike anything I’ve seen while touring other residential facilities. We’re a very much a community—a diverse community. That’s where a lot of the power is.
MW: You’ve worked here since this place first opened. It’s grown quite a lot since then?
DC: Oh, yeah.
MW: How is that changing your job?
DC: Driftwood’s growth has felt like a managed, gradual process. We’ve been able to on more staff, or add more programs, at the moments when we’ve needed them. So it doesn’t feel like there’s been a whole lot of abrupt change. We’re a well-oiled machine. But we’ve had to be flexible in our thinking—open to new ideas and systems. In the beginning, we didn’t need a lot of that, because the place was so small.
MW: Can you give an example of a system that you might have been reluctant to put in place initially, but that you’re using now?
DC: I was thinking mainly of the systems we use for communication. In the early days of Driftwood, the care coordinators were able to just talk to one another about anything important. We’ve retained that family feeling, but now, for instance, we do use Slack to make sure that everyone is up to speed on everything.
But what’s more striking to me is how many things are remaining the same. I truly believe the leadership team when they promise that we’re never going to lose our culture. I believe that.
MW: What are some of the features of that culture that you’ve seen that seem especially important to you—things that, if they disappeared, would be a real loss?
DC: At Driftwood, the staff and residents always eat meals together, we do a lot of things together, and we don’t ever want the clients to feel like the staff is separate from them. It’s very integrated. We know so much about every client, and work so much on each case. What we offer is very individualized, in part because we have the time and staffing to do that. No one’s ever going to be just a number here. We get creative with every treatment plan, with every discharge plan.
MW: Is there a time of day, or of the week, when the care coordinators get together to share their experiences with one another, to offer moral support, and so on?
DC: Not exactly, because we’re all so close. We do have care-coordinator meetings. But we also have three people working together on every shift. So that kind of moral support is naturally given every day, every shift.
MW: If someone was considering residential treatment here—for themselves or for a loved one—what’s the thing you’d most want them to know?
DC: When I came into recovery, I only learned one set of strategies, one set of ideas about addiction and sobriety, and they happened to work very well for me. So I came to Driftwood not knowing much about the clinical side of the programs here. This place has taught me that there are multiple pathways to long-term sobriety. Meeting people where they’re at, that’s what guides people into long-term sobriety, right? What worked for me might not work for another person. But something is going to work for them, and the staff at Driftwood is going to be patient and curious and compassionate enough to help them find that thing.
“Some trainers have one way to do something. But every client is different. Each body is weak and strong in different ways. I see that uniqueness in the residents who stay at Driftwood.”
“Everything Was Preparing Me to Be Right Here, Right Now”
This is the fourth in a series of posts introducing the people who make up Driftwood Recovery’s community of caregivers.
Through these conversations, you’ll get a chance to meet the people on Driftwood’s team—from its executives to its care coordinators. You’ll learn about the programs they facilitate, and about how their work serves Driftwood’s overall treatment philosophy. You’ll learn about the various paths that brought them here. And you might pick up a book or Austin restaurant recommendation.
In this post, Kuraĝo editor Matt Williamson talks with Driftwood’s Wellness Director, Connie Cole (CPT, CHC, CYI), and Ryan Potter, a health coach in the Wellness Center.
***
Matt Williamson: Connie, you’ve been at Driftwood from the beginning, right?
Connie Cole: I was here before the beginning! This place was a bed and breakfast. And I helped design the Wellness Center.
I was working as a personal trainer, and one of my clients was the woman who was building this place. I mentioned to her that I was in the process of selling my studio. And she was like: “Oh, I’m building a gym. You should train your clients out there, and you can train me, too. We’ll work out some deal.” I had no idea that she was building this beautiful facility. She was in the process of turning a raccoon-infested house into a state-of-the-art gym, building it up. I ended up working out here as a trainer for four years. And then she decided to sell the place.
When she sold, I was like, “oh, no—what am I going to do?” But then Driftwood Recovery’s founders came out, and I happened to meet them. They had several months of preparatory work left to do, and they said: “you don’t have to leave. Just keep meeting your clients out here until we open. It’s no problem.” They didn’t know me from the man in the moon.
Then I started training them. They discovered that my specialty was working with people with disease and disability: chronic pain, bad shoulders, a bad back, bad knees. So they hired me. For the first year and a half, I helped them develop Driftwood’s wellness program. And then we hired Ryan because we were growing so fast. I’m here full time, and Ryan comes in from one to five. That’s when a lot of the activity happens—in the afternoon.
MW: Ryan, what were you doing before you came out here?
Ryan Potter: I was at UT, studying kinesiology. While I was a student, I worked for the men’s basketball program. I was a strength intern. I facilitated and administered training regimens. That could mean something as simple as changing weights, or it could mean workshopping an entire strength program with a student athlete. During the summer and offseason, we did a lot of stretching. I found out that stretching the leg of a seven-foot-tall athlete is a three-man job.
The guys that were our strength coaches there have gone on to bigger things. One of them is coaching for the Philadelphia 76ers. Another one is an associate professor at a university. So even outside of class, I was learning from highly accomplished, deeply knowledgeable people.
A lot of that work at UT involved rehabbing injuries, teaching people how to work around injuries. That all became directly relevant to the work I’m doing now at Driftwood.
MW: Connie, what got you interested in working with people in chronic pain?
CC: I started out as a martial artist thirty years ago. And my master was hurting people. We were using our body weight to train, and he was popping Achilles tendons, breaking shoulders. I kept thinking: there’s got to be a way to do this without injury. That’s how I initially became interested in training: I wanted to become a better athlete without hurting myself.
But when I started working as a trainer, every client seemed to have a bad back, or some other ailment. Because I wanted to help them, I started studying ways of training people for function, training them to feel better. The transition to my current chronic pain specialization was very natural.
MW: I had this personal trainer a few years back who was a former Big Ten football player. And this guy did not understand my limits at all. He wanted me to do all of this stuff that I wasn’t comfortable with. Even if everything was safe—I’m sure it was—it didn’t feel safe. I kept trying to make him understand that I wasn’t hoping to compete on American Ninja Warrior; I just wanted to be in slightly better shape! I wish I’d worked with you two instead.
CC: Some trainers have one way to do something. But every client is different. Each body is weak and strong in different ways. I see that uniqueness in the residents who stay at Driftwood. We get people who are extraordinarily conditioned—over-conditioned, even. We get people who are in wheelchairs, or who have been run over by cars, who are in pain in ten different places in their body.
My background has helped me deal with that variety. In a way, I feel that for my whole life, I was training to do this job—like everything I did was preparing me to be right here, right now. I’m doing my dharma. This is what I love.
MW: What do you mean by “over-conditioned?”
CC: You’ve heard of cross addiction. We have people out here, sometimes, who are addicted to exercise. They’re not necessarily bodybuilders, and they don’t necessarily have body-image problems; they just have to exercise every day, to an unhealthy degree. You should exercise every day! But that doesn’t mean you should do CrossFit every day.
MW: Why not?
CC: If someone took a bat right now, and lightly beat you all over your body, your body would produce free radicals. A lot of inflammation happens. Your body would be in disrepair.
Something similar happens with your entire body is overworked through exercise. Did you get that soreness from being beaten up, or from overexertion? Your body doesn’t know the difference. Many of the same physiological results happen.
MW: How do you customize a fitness program for a new resident?
CC: Every resident that comes here—whether they’re on the pain track, or on the chemical dependency track—gets an assessment by me. People in the pain program get a more thorough evaluation, because they need it. They also get evaluated by our medical director. They get evaluated by our nurse practitioner. They get evaluated by Dr. Melanie Somerville. Then we all collaborate on how best to get them out of their pain or get them functional without whatever substances they were using.
MW: What are you literally doing during that initial assessment?
CC: I jokingly refer to it as a Vulcan mind-meld. I try to find out as much as I can about their pain. Is it localized, or is it a systemic inflammatory pain, like Crohn’s disease? A person might come in with pain from a traumatic brain injury. I ask where they’re feeling the pain, and they show me.
At that early stage, we won’t use weights or anything like that. We’re just talking. Sometimes we will move. My goal, sometimes, is to see how I can shift someone from lying down or sitting to moving.
But it’s very low key. It’s copacetic. It’s not scary. It’s not hard. It’s not threatening. It’s kind of fun. “What do you like? What do you dislike?”
Later, when residents come here and start exercising, it’s never intimidating. People can work out with Ryan and do some of the harder things, or they can walk, or they can ride their bike, or they can swim.
RP: Connie and I know that we have a limited window of time with all the clients here. Part of my job is planning an individualized program that will get a client to the goals that they want to achieve in X amount of time. In athletics, that’s super important, because you have a start date on the season: here’s where this athlete is, we need to get them ready by this point.
In certain ways, the situation is similar when it comes to new residents at Driftwood who will be transitioning out of here in one or two months. We want to get them ready for the next phase of their lives.
MW: How much time generally passes between the end of someone’s detox and the beginning of their sessions with the two of you?
CC: Most people who come here have about a week of detox, although that period varies, depending on how you feel, and how you are detoxing. During your detox, you may or may not want to participate in our fitness programs. If you don’t want to move or exercise during that first week, you don’t have to. But we might encourage you to move.
The phrase we use at Driftwood is “challenge by choice.” I’m not going to tell you that you have to do high intensity interval training with Ryan. You get to pick your challenge. If you can drag yourself down to the gym and put one foot in the door and do a little something, I promise that when you leave, you’ll feel better. You’ll feel better every time.
RP: Just to give an example of challenge by choice: lately I’ve been taking control of the afternoon group exercise. And over the course of the last two or three cohorts, it’s evolved into a full-fledged workout. But it changes from class to class. It’s scalable. And you can always join a group exercise but work at your own pace.
We put a menu of exercises up on the wall every single day. If you can complete every single one of these, that’s amazing. We’re proud of you. But if you come in and just try a couple of them, we’re happy with that too.
MW: Why is it important to have not just “a gym” but “a wellness center?” I’ve heard clinicians describe the work that you and Ryan are doing as fundamental to the broader recovery project here.
CC: Everyone at Driftwood believes that fitness, and being functional, is vital to being sober. If you’re not moving every day, you’re degenerating. On the other hand, when you move every day, your body starts to function better, your mind functions better, and you start to feel better. And when you feel better, you don’t feel like you’re seen in the same way. Having a spring in your step, feeling strong and empowered, helps you stay sober and helps you in your life outside of recovery.
MW: Could you discuss the concept of aftercare? How can people sustain and deepen their wellness when you and Ryan aren’t around?
CC: Good question. While you’re here, of course, you get to exercise every day. You have wonderful food every day, and meaningful clinical therapy every day. It’s a healthy bubble, and you’re scheduled in that bubble. But you’re also becoming equipped to stay healthy when you integrate back into the world.
Many of our residents transition to our Riverside extended care facility. Everyone who goes to Riverside gets a membership at the Y downtown, and our house manager Cassie encourages them, finds a way for them to exercise regularly. Ryan, on his own time, trains a lot of people who are in that community integration program. If he’s developed a strong relationship with someone, he’ll try to continue working with them after they leave.
MW: I’d like to finish with an open-ended question for both of you. Could you share something that you think people should know about the Wellness Center? Something, maybe, that I should have asked you about, but didn’t?
RP: One thing that’s great about this place is the fact that Connie and I have complementary skill sets. In addition to the background she’s already described—all of those certifications she has—she’s also a yoga instructor. I’m certified in a technique called foundation training, which is for lower back health and core strength. I’m one of the few people in Austin that has that certification. Between the two of us, we’re ready for almost anything.
CC: I said earlier that I feel I’m “doing my dharma” here at Driftwood. Dharma is about whether you’re doing what you were put on this planet to do. Are you living your dream? Are you doing what you’re good at? One of our goals is to find that thing for the residents. Maybe they’ve lost it, or maybe they’ve never found it.
We’ve had people who have left here who have gone on to be personal trainers. They had such a positive experience with us that our work became part of their dream. Some people leave here and find their dharma by becoming therapists in the recovery community. A lot of the people who work at Driftwood are in recovery. They’re here because they want to help people who have been in the same shoes that they’ve been in.
We work with people on this crucial question: what meaningful role are you going to have in the world when you leave here? And sometimes, people find that through fitness.
Contact us

Break the cycle of suffering through surrender.
Contact Driftwood Recovery today to get more information or schedule a tour.